LEAN SIX SIGMA FOR HOSPITALS
One Lean leader.One application.Every contributor at Yellow Belt level.
LeanColab digitizes the existing continuous improvement program — DMAIC, Lean, Kaizen — without replacing it. Meetings stop being catharsis and become decision-making.
- Free sandbox
- No credit card
- EU data residency
BUILT BY PHYSICIANS WITH ACTIVE HOSPITAL PRACTICE IN PORTUGAL AND EUROPE
Dr. Hugo Viegas (CEO) · Dr. Gonçalo Mendes (Managing partner)
THE DIAGNOSIS
Whoever leads continuous improvement in a private hospital is losing more time documenting than improving.
The Lean leader is a Green or Black Belt — rare training, hard-to-obtain certification, years of practice to master DMAIC. But the team that needs to apply it every day — nursing, technicians, administrative staff — has never had White or Yellow Belt. The program doesn't fail for lack of methodology. It fails because only one person knows how to apply it.
What is lost without a dedicated tool
- The continuous improvement program runs on Excel, Word, email and PowerPoint.
- 5 Whys and Ishikawa analyses live in local files — no traceability, no reuse.
- Each DMAIC project takes 6 to 9 months to close and is rarely cited again.
70%
OF LARGE-SCALE CONTINUOUS IMPROVEMENT INITIATIVES FAIL
McKinsey & Company, cited in QI healthcare literature
50%
OF CONTINUOUS IMPROVEMENT STUDIES PRODUCE NO CHANGE IN CLINICAL PRACTICE
Ivers et al., J Gen Intern Med 2014, 25-year meta-analysis
As a physician, I know well what clinical meetings look like — disorganized, everyone doing catharsis and complaining, with no decision. Meetings should serve to aggregate already-characterized problems and decide on solutions. LeanColab removes that friction from the meeting.
— Dr. Hugo Viegas, CEO LeanColab
The literature confirms what clinicians feel every day: teams that report problems and don't see action taken progressively reduce the number of reports. It isn't disinterest — it is operational learning about what is worth reporting.
- In Portugal, only 22% to 50% of clinical incidents are ever reported, depending on context¹.
- Only 32% to 65% of incoming reports contain actionable information about root causes².
- 53.2% of adverse events in Portuguese hospitals are preventable³.
¹ Yung et al., scoping review, Healthcare 2024 — rates vary between 22-50%.
² SAFE Loop trial (Cedars-Sinai, NCT05381441).
³ Sousa et al., Pilot study of adverse event incidence in Portuguese hospitals, ENSP/NOVA, 2011.
THE SOLUTION
LeanColab digitizes the existing continuous improvement program. Without replacing it.
We are not Lean consultants. We will not teach DMAIC to those who have practiced it for years. We give the tool that was missing to apply it at team scale, and free meetings from catharsis into decision-making.
THE LEAN LEADER REMAINS SOVEREIGN
The Green or Black Belt remains the owner of the methodology, of the committees, of the program roadmap. LeanColab does not replace anyone — it multiplies.
- Keeps DMAIC, Lean, Kaizen as before
- Configures LSS toolkits according to project phase
- Runs committees with data, not guesswork
EVERY CONTRIBUTOR AT YELLOW BELT LEVEL
The 50, 100 or 300 contributors stop being passengers — they contribute every day. No certification, no extensive training, no friction.
- Identifies muda the moment it occurs
- Applies 5 Whys with a guided wizard
- Submits solutions in the internal forum
MEETINGS BECOME DECISION-MAKING
Problems arrive at the meeting already characterized, with root causes already analysed, with solutions already voted by the team. What's left are decisions — not venting.
- Agenda generated automatically from the week's work
- Visible status of every project in flight
- Decisions recorded and traceable over time
Contributors don't need to know what DMAIC is. They only need to know what they saw. LeanColab translates operational observation into the Lean structure, and returns to the program leader material already organized for analysis.
HOW IT WORKS
The full cycle: capture → analyse → decide.
In three screens you see how a problem observed by an operational assistant arrives at the quality committee meeting already structured and prioritized.
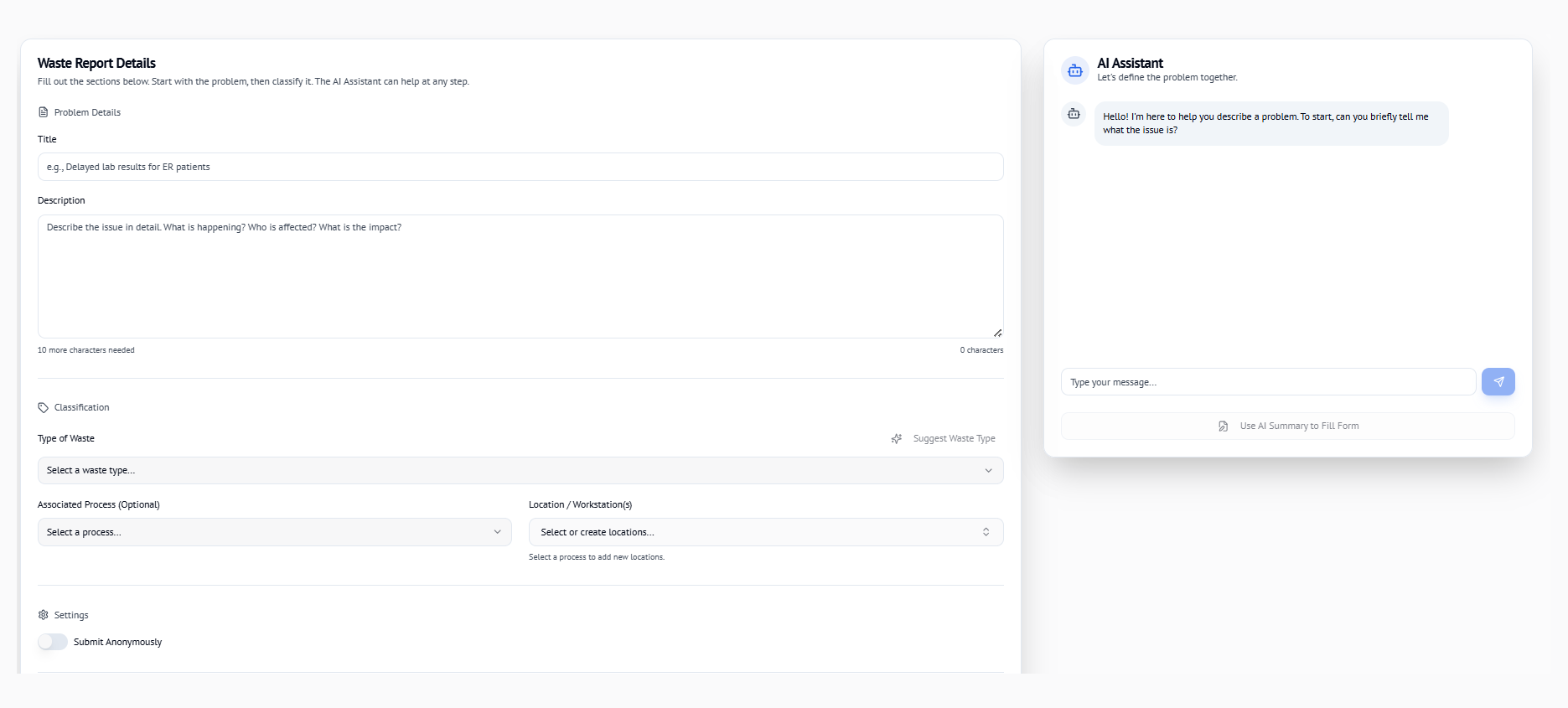
01
CAPTURE
The contributor sees something wrong. Opens the app on her phone. Clicks a button. LeanColab guides her with simple questions: what she saw, where, when. It automatically classifies the DOWNTIME muda.
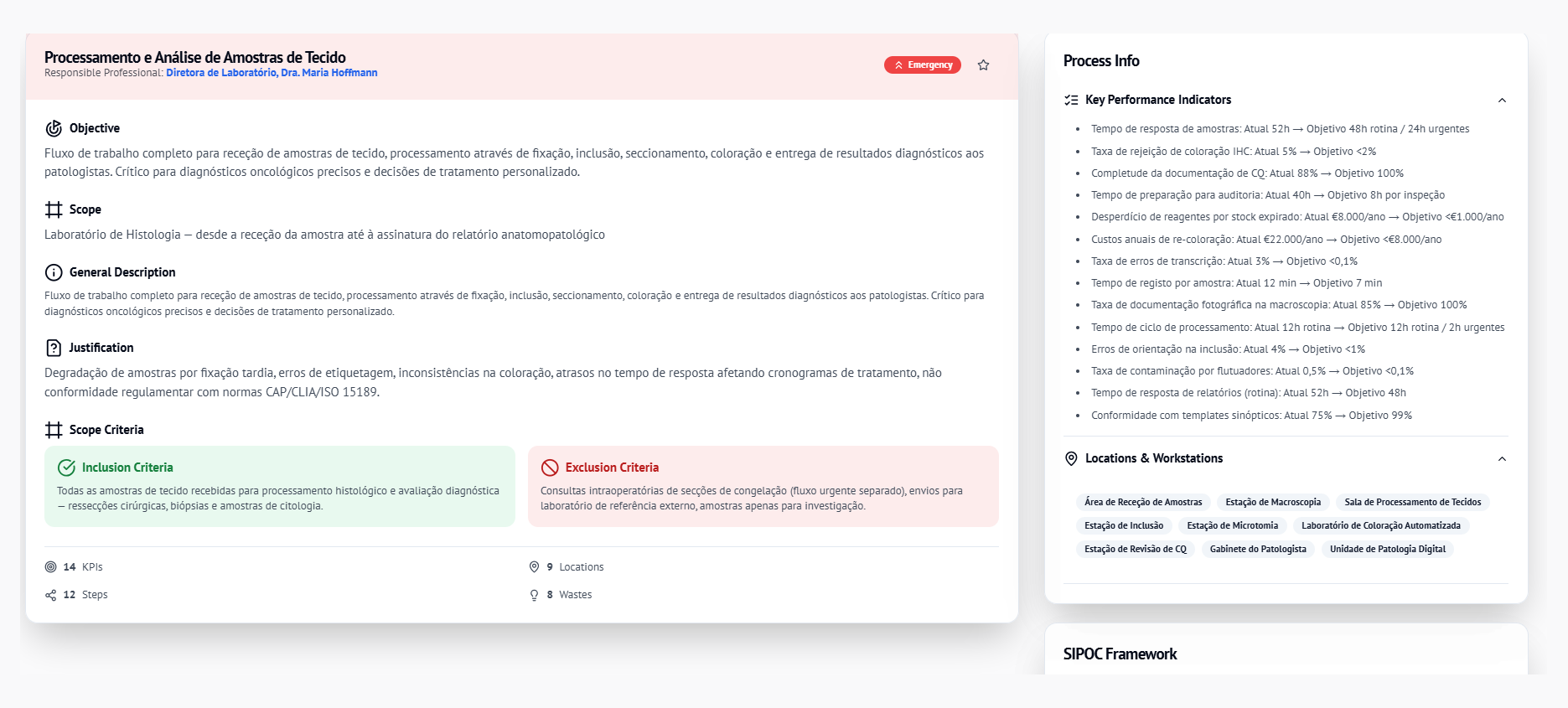
02
ANALYSE
The program leader opens the weekly backlog. Reports arrive structured. Applies 5 Whys or Ishikawa with a wizard. The AI suggests root causes and patterns based on the hospital's history — always with human supervision.
03
DECIDE
The meeting opens with the aggregated dashboard: muda by service, most frequent root causes, projects in flight, success rate. Recorded decisions are traceable. No catharsis. No PowerPoint. No re-doing work.

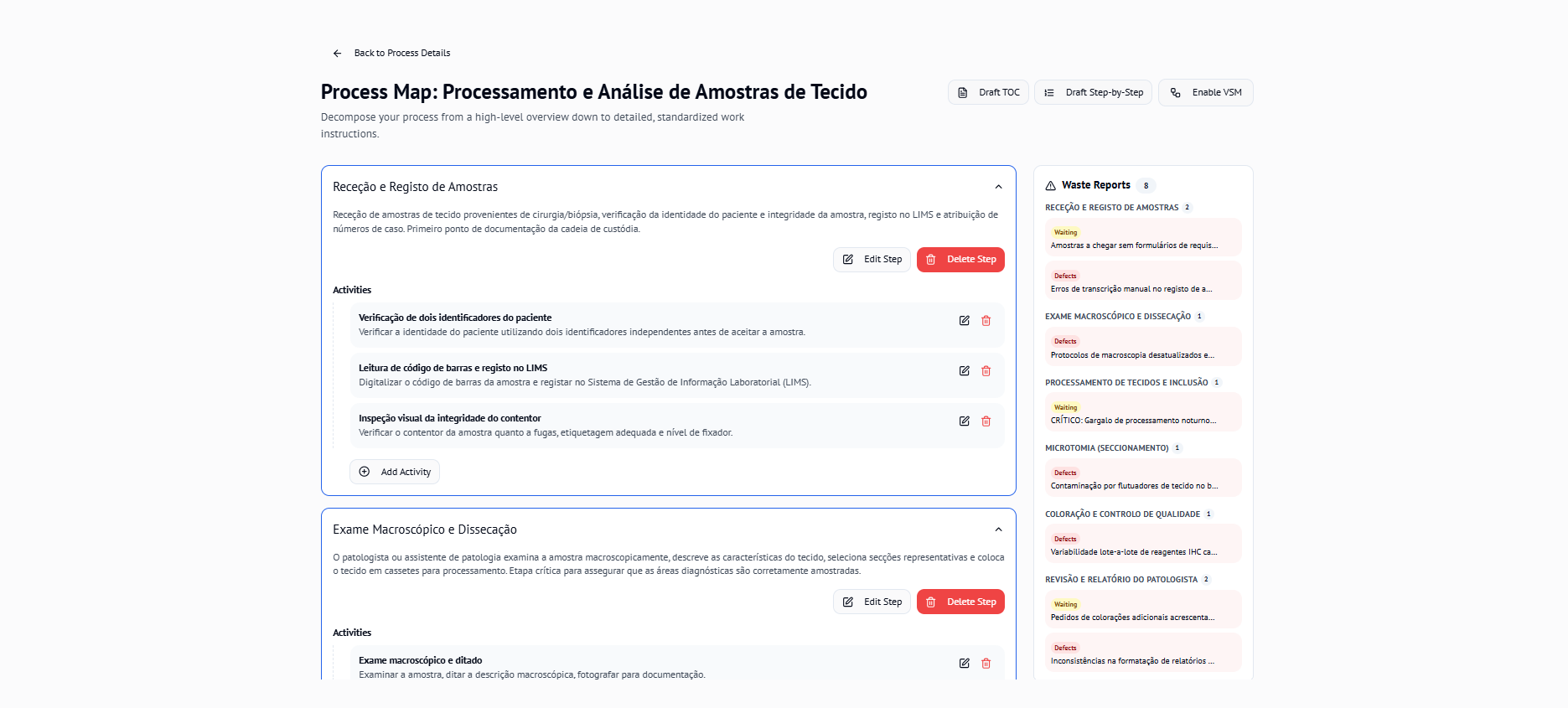
VALUE STREAM MAPPING
See the full patient journey — waste and all.
LeanColab's VSM tool lets quality leaders map every step of a care pathway, identify non-value-adding activities, and build a future-state vision — collaboratively, in real time.

Live collaboration
Multiple team members edit the same map simultaneously. Changes sync instantly — no emailing files back and forth.
Waste highlighted automatically
DOWNTIME categories are flagged on each step as the team builds the map, turning an abstract exercise into actionable data.
Current state → future state
Export or present the before/after view in the committee meeting. Track improvement targets over time.
DIAGNOSIS
Where does your hospital's continuous improvement program stand?
Answer 4 questions. In 90 seconds you find out the conversion rate of your program, the gap to scientific literature, and the cost of the gap in euros.
AVERAGE CONVERSION RATE WITHOUT A DIGITAL TOOL
<30%
McKinsey & Ivers et al., 2014
PREVENTABLE ADVERSE EVENTS IN PT HOSPITALS
53.2%
Sousa et al., ENSP/NOVA, 2011
AVERAGE COST OF AN ADVERSE EVENT PER EPISODE
€4,436
Costa et al., RPSP, 2011
ANNUAL COST OF ADVERSE EVENTS IN THE PORTUGUESE NHS
>€100M
CINTESIS, J Medical Systems, 2018
HOW WE CALCULATE
For a typical hospital, the formula combines: beds × occupancy × adverse-event incidence (CINTESIS, 2018), average cost per event (Costa et al., RPSP), documented preventability rate (Sousa et al., ENSP), current conversion rate of your program (input). The result is a defensible range, not a promise. Real gain depends on implementation.
But the cost is not just financial. Every improvement not acted upon is a frustration for whoever reported it. The literature is clear: teams that report and don't see action taken progressively reduce the number of reports. It is the 'innovation fatigue' described by Flynn et al. (2018) — not disinterest, but operational learning about what is worth reporting.
The real cost is the loss of the habit of improving.
— Dr. Hugo Viegas, CEO LeanColab
4 questions · 90 seconds · result with literature references
FOR ADMINISTRATION AND CLINICAL LEADERSHIP
Compliance, data residency, and adoption roadmap.
LeanColab was built with the requirements of a European private hospital in mind: GDPR, AI Act, EU residency, and phased implementation that doesn't require reforming anything before starting.
GDPR AND AI ACT COMPLIANCE
All infrastructure runs on European data residency (Vertex AI europe-west4). The AI has guardrails — no autonomous clinical decision, mandatory human supervision, auditable log of every action. Technical documentation compliant with AI Act 2026 and GDPR.
PHASED INTEGRATION, NO BIG BANG
Tier 0: QR codes, no integration at all. Tier 1: REST API. Tier 2: SClínico and Glintt HS connectors. Tier 3: FHIR/HL7. Each hospital chooses the right depth for its IT-maturity level.
ACCREDITATION AND AUDIT
Evidence packs ready for JCI, JC, KTQ, DGS. Centralized audit logs with sanitization. Reports for leadership generated from real activity, not built manually in PowerPoint.
Want to present LeanColab to your hospital's leadership?
Book 30 min with Dr. Hugo Viegas →GETTING STARTED
Free sandbox today. Paid plan when the service is already using it.
Every user starts on Family — individual sandbox, no clinical data, no card. When you're ready for your team, you upgrade inside the app without friction.
FREE
€0
No time limit
Individual sandbox to try the product. No clinical data, no PHI, no DPIA.
- 1 user, 1 VSM
- Essential Lean toolkit
- Basic AI (3 flows)
FOR ONE TEAM
€55/month
€660/year
The first clinical team in your hospital, in one service.
- 5 Leader seats
- Unlimited contributors in the team
- VSM with basic API integration
- Mobile + QR muda capture
FOR A PROGRAM
€144/month
€1,728/year
Multiple services, advanced AI, customizable dashboards.
- 10 Leader seats
- Unlimited contributors
- Patient Journey Tracker
- FMEA, SPC, Pareto
- Advanced AI (19 flows)
Larger health system, FHIR integration, or accreditation packs?
SECURITY AND COMPLIANCE
Built for what a European private hospital requires.
European data residency, AI with guardrails, centralized audit logs, and technical documentation compliant with AI Act 2026 and GDPR. Compliance is not a feature — it is a precondition.
EU DATA RESIDENCY
Vertex AI in europe-west4. Firestore in European region. No data transfer outside the EU.
AI WITH GUARDRAILS
No autonomous clinical decision. Mandatory human supervision. Every AI action is recorded and auditable.
CENTRALIZED AUDIT LOGS
Every access, every change, every decision is recorded. Automatic sanitization of sensitive data.
DOCUMENTATION READY
AI Act technical pack, GDPR policy, BAA/DPA templates, data-processing maps — available at any time.
Available technical documentation:
GDPR PolicyAI Act ClassificationBAA/DPA TemplateData Retention PolicyFAQ
Questions hospital teams ask
What is LeanColab?
LeanColab is a healthcare Lean Six Sigma platform that digitizes your hospital's existing continuous-improvement program. Every contributor — nurses, technicians, porters, administrators — participates at Yellow Belt level while one Lean leader runs the DMAIC cycle.
Do we have to replace our current improvement program?
No. LeanColab digitizes the program you already run instead of replacing it, so your meetings stop being catharsis sessions and turn into tracked decisions and actions.
Do I need Green Belt or Black Belt certification to use it?
No. The platform is built so any frontline contributor can report waste and propose improvements at Yellow Belt level, while a single trained Lean leader steers the structured analysis.
How much does LeanColab cost?
There is a free Family tier, a €55/month Starter tier, and a €144/month Professional tier, plus a custom Hospital tier for whole-hospital deployments. Frontline contributors are unlimited on every paid tier.
Where is our data stored and is it GDPR compliant?
All data is processed and stored in the European Union (europe-west4). LeanColab is GDPR-compliant by default and HIPAA-aligned, with audit trails and EU data residency.
Which languages does LeanColab support?
LeanColab is available in Portuguese, English, and Spanish.
One Lean leader. One application. Every contributor at Yellow Belt level.
Start trying it now. If you see potential, we'll book a session to help with advanced configurations, or to present together to leadership.
Free sandbox · No credit card · No internal approval